
 By B.N. Frank
By B.N. Frank
Decades of peer-reviewed published research has determined that exposure to radiation from cell phones (and cordless landline phones) is biologically harmful. In fact, manufacturers are required to provide warnings about exposure risks for all wireless radiation emitting products. In some countries, government agencies actually warn residents about this. Nevertheless, there are researchers who continue to publish studies dismissing exposure risks which also leaves them wide open for expert criticism.
Thanks to Lennart Hardell and Joel M. Moskowitz for their take on the MOBI-Kids Study:
MOBI-KIDS: Childhood Brain Tumor Risk & Mobile Phone Use Study
A critical analysis of the MOBI-Kids study of wireless phone use in childhood and adolescence and brain tumor risk
Lennart Hardell, Joel M. Moskowitz. A critical analysis of the MOBI-Kids study of wireless phone use in childhood and adolescence and brain tumor risk. Reviews on Environmental Health. May 5, 2022. https://doi.org/10.1515/reveh-2022-0040.
Abstract
The MOBI-Kids case-control study on wireless phone use and brain tumor risk in childhood and adolescence included the age group 10–24 years diagnosed between 2010 and 2015. Overall no increased risk was found although for brain tumors in the temporal region an increased risk was found in the age groups 10–14 and 20–24 years. Most odds ratios (ORs) in MOBI-Kids were <1.0, some statistically significant, suggestive of a preventive effect from RF radiation; however, this is in contrast to current knowledge about radiofrequency (RF) carcinogenesis. The MOBI-Kids results are not biologically plausible and indicate that the study was flawed due to methodological problems. For example, not all brain tumor cases were included since central localization was excluded. Instead, all brain tumor cases should have been included regardless of histopathology and anatomical localization. Only surgical controls with appendicitis were used instead of population-based controls from the same geographical area as for the cases. In fact, increased incidence of appendicitis has been postulated to be associated with RF radiation which makes selection of control group in MOBI-Kids questionable. Start of wireless phone use up to 10 years before diagnosis was in some analyses included in the unexposed group. Thus, any important results demonstrating late carcinogenesis, a promoter effect, have been omitted from analysis and may underestimate true risks. Linear trend was in some analyses statistically significant in the calculation of RF-specific energy and extremely low frequency (ELF)-induced current in the center of gravity of the tumor. Additional case-case analysis should have been performed. The data from this study should be reanalyzed using unconditional regression analysis adjusted for potential confounding factors to increase statistical power. Then all responding cases and controls could be included in the analyses. In sum, we believe the results as reported in this paper seem uninterpretable and should be dismissed.
Summary
- In our opinion, the results as reported in the MOBI-Kids paper seem uninterpretable and should be dismissed.
- All brain tumor cases should have been included regardless of histopathology and anatomical localization.
- Only surgical controls with suspected appendicitis were used. Yet, increased incidence of appendicitis has been postulated to be associated with RF radiation.
- Start of wireless phone use up to 10 years before diagnosis was in some analyses included in the unexposed group. This would bias the ORs towards unity.
- The results indicate an increased risk for tumors in the temporal brain region in spite of methodological issues based on low numbers in several categories.
- Linear trend was in some analyses statistically significant in the calculation of RF-specific energy and ELF-induced current in the center of gravity of the tumor. Additional case-case analysis should have been performed.
- The data from this study should be reanalyzed using unconditional regression analysis adjusted for potential confounding factors to increase the statistical power.
Finally, it is unfortunate that after such a major investment of resources that little can be learned at this time from the MOBI-Kids study about the risk of brain tumors from wireless phone use in young people. Since the study addresses an issue critical to public health and the majority of the funding was from the European Commission, the MOBI-Kids data set should be publicly archived making it available to the scientific community to enable the data to be re-analyzed using different assumptions and methods.
Open access paper: https://www.degruyter.com/document/doi/10.1515/reveh-2022-0040/html
—
Feb 2, 2022
My Comments on the International MOBI-Kids Study
In December 2021, almost seven years after data collection was completed, the main outcome paper for the International MOBI-Kids study was finally published. This case-control study examined brain tumor risk from wireless phone use among young people 10-24 years of age (Castaño-Vinyals et al, 2022) (see abstract below).
Conducting a multinational epidemiologic study involving more than 50 scientists with data collected in 14 nations is a complex endeavor with a substantial risk of failure. Although the investigators made an exemplary effort to salvage the study via supplemental sub-studies and post-hoc analyses, after reviewing their paper, we believe they were unsuccessful in overcoming serious methodological problems. Hence, in our opinion, the data seem uninterpretable, and the study’s results should be dismissed.
The authors of the MOBI-Kids study appear to agree with our assessment because they concluded in the paper’s abstract:
“Further analyses suggest that the large number of ORs below 1 in this study is unlikely to represent an unknown causal preventive effect of Mobile phone exposure: they can be at least partially explained by differential recall by proxies and prodromal symptoms affecting phone use before diagnosis of the cases. We cannot rule out, however, residual confounding from sources we did not measure.
Overall, our study provides no evidence of a causal association between wireless phone use and brain tumours in young people. However, the sources of bias summarised above prevent us from ruling out a small increased risk.”
Based upon our review of the research on brain tumor risk among adults who use mobile phones (Choi et al., 2020), we recommend that those who must use mobile phones should keep their use as low as reasonably achievable (ALARA) and should follow safety guidelines. These guidelines especially apply to children and adolescents whose brains and bodies are still developing.
Specific concerns re: the MOBI-Kids study methodology
We believe there is an explanation for the many risk estimates less than 1 in the MOBI-Kids study. The study had substantially lower participation rates for controls (54%) than cases (72%) that likely biased brain tumor risk estimates downward. The investigators conducted a non-participation study to estimate the amount of this bias, but this study also had serious limitations (i.e., small sample sizes; differential participation rates) and likely underestimated the amount of selection bias in the current paper.
The original study design called for recruitment of 2,000 cases (Sadetzki et al., 2014). Due to problems with recruitment, the study managed to enroll only 898 cases. Moreover, the primary analyses in the outcome paper included only 671 cases with neuroepithelial brain tumors (NBT). Hence, the study had inadequate sensitivity (i.e., statistical power) to detect even a moderate-sized effect (let alone a small effect) from mobile phone use on brain tumor risk.
In a case-control study, controls should be selected that have equal risk for the study outcome as the cases. We question whether using youth diagnosed with appendicitis as controls constitutes a suitable choice for a study of cell phone users. Why didn’t the study include a population-based control group like the INTERPHONE study which preceded it (Cardis et al., 2007)?
During the data collection period (2010-2015), many young people in this study may have used smart phones. Whereas earlier cellphones had antennas at the top of the phone, many smart phones have cellular transmission antennas in the bottom of the phones exposing the neck to the greatest radio frequency radiation, not the head. This may increase the risk of other tumors, especially thyroid gland tumors, but reduce the brain tumor risk.
Finally, ten or fewer years of mobile phone use may not be a sufficient amount of time before a mobile phone-related brain tumor is diagnosed in this young population. However, the CEFALO study (Aydin et al., 2011) of children’s mobile use and brain tumor risk did find a significant dose-response relationship for the number of years of cellphone use in a subsample of participants with mobile phone operator (i.e. telephone company) data. The MOBI-Kids study also had mobile phone operator data on 25% of participants but did not report the outcome results for this subsample.
MOBI-Kids and CEFALO differed in important ways. MOBI-Kids used hospital controls whereas CEFALO selected controls from the general population. Whereas MOBI-Kids included only neuroepithelial brain tumors (NBT) in its primary analyses, CEFALO did not exclude any brain tumors. MOBI-Kids collected data years later when different cellular technology was popular, and mobile phone towers likely were located more proximal to users which may have resulted in less exposure to RFR emitted by cellphones. Although MOBI-Kids collected data in 14 countries, most of the data were from five countries, Spain, Italy, France, Israel, and Germany, and none was from the four CEFALO countries, Denmark, Norway, Sweden, and Switzerland.
In sum, it is unfortunate that after such a major investment of resources and time that little can be learned from the MOBI-Kids study about the risk of brain tumors from wireless phone use in young people. Since the study addresses an issue critical to public health and the majority of the funding was from the European Commission, the MOBI-Kids data set should be made available to the scientific community for secondary analysis to enable the data to be re-analyzed using different assumptions and methods.
—
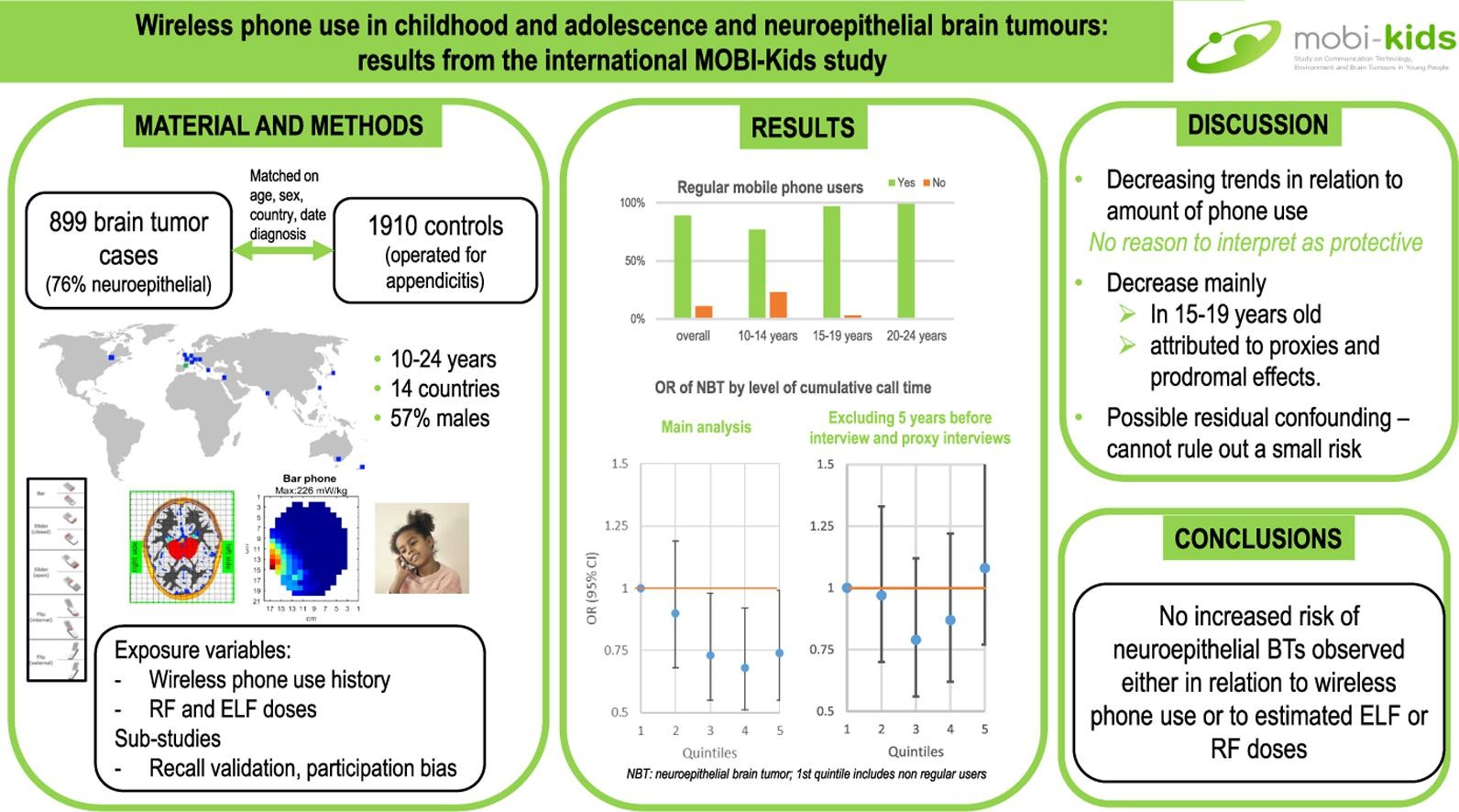
Wireless phone use in childhood and adolescence and neuroepithelial brain tumours: Results from the international MOBI-Kids study
Castaño-Vinyals G, Sadetzki S, Vermeulen R, Momoli F, Kundi M, Merletti F, Maslanyj M, Calderon C, Wiart J, Lee AK, Taki M, Sim M, Armstrong B, Benke G, Schattner R, Hutter HP, Krewski D, Mohipp C, Ritvo P, Spinelli J, Lacour B, Remen T, Radon K, Weinmann T, Petridou ET, Moschovi M, Pourtsidis A, Oikonomou K, Kanavidis P, Bouka E, Dikshit R, Nagrani R, Chetrit A, Bruchim R, Maule M, Migliore E, Filippini G, Miligi L, Mattioli S, Kojimahara N, Yamaguchi N, Ha M, Choi K, Kromhout H, Goedhart G, ‘t Mannetje A, Eng A, Langer CE, Alguacil J, Aragonés N, Morales-Suárez-Varela M, Badia F, Albert A, Carretero G, Cardis E. Wireless phone use in childhood and adolescence and neuroepithelial brain tumours: Results from the international MOBI-Kids study. Environ Int. 2021 Dec 30;160:107069. doi: 10.1016/j.envint.2021.
Abstract
In recent decades, the possibility that use of mobile communicating devices, particularly wireless (mobile and cordless) phones, may increase brain tumour risk, has been a concern, particularly given the considerable increase in their use by young people. MOBI-Kids, a 14-country (Australia, Austria, Canada, France, Germany, Greece, India, Israel, Italy, Japan, Korea, the Netherlands, New Zealand, Spain) case-control study, was conducted to evaluate whether wireless phone use (and particularly resulting exposure to radiofrequency (RF) and extremely low frequency (ELF) electromagnetic fields (EMF)) increases risk of brain tumours in young people. Between 2010 and 2015, the study recruited 899 people with brain tumours aged 10 to 24 years old and 1,910 controls (operated for appendicitis) matched to the cases on date of diagnosis, study region and age. Participation rates were 72% for cases and 54% for controls. The mean ages of cases and controls were 16.5 and 16.6 years, respectively; 57% were males. The vast majority of study participants were wireless phones users, even in the youngest age group, and the study included substantial numbers of long-term (over 10 years) users: 22% overall, 51% in the 20-24-year-olds. Most tumours were of the neuroepithelial type (NBT; n = 671), mainly glioma. The odds ratios (OR) of NBT appeared to decrease with increasing time since start of use of wireless phones, cumulative number of calls and cumulative call time, particularly in the 15-19 years old age group. A decreasing trend in ORs was also observed with increasing estimated cumulative RF specific energy and ELF induced current density at the location of the tumour. Further analyses suggest that the large number of ORs below 1 in this study is unlikely to represent an unknown causal preventive effect of mobile phone exposure: they can be at least partially explained by differential recall by proxies and prodromal symptoms affecting phone use before diagnosis of the cases. We cannot rule out, however, residual confounding from sources we did not measure. Overall, our study provides no evidence of a causal association between wireless phone use and brain tumours in young people. However, the sources of bias summarised above prevent us from ruling out a small increased risk.
Highlights
- Increasing use of mobile technologies by young people is a topic of public health concern.
- MOBI-Kids studied brain tumour risk and wireless phone use (and EMF) in 14 countries.
- The study includes 899 brain tumour cases aged 10–24 years old and 1,910 controls.
- We have no evidence of a causal association between wireless phone use and brain tumours.
- Because of likely biases we cannot rule out a small increased risk.
Open access paper: https://www.sciencedirect.com/science/article/pii/S0160412021006942?via%3Dihub
==
February 18, 2021
When will we learn whether mobile phone use was associated with increased risk of brain tumors or neurological disorders in the Mobi-Kids study?
February 15 was #InternationalChildhoodCancerDay which reminded me that we have yet to see publication of the most important results from the Mobi-Kids Childhood Brain Tumor Risk & Mobile Phone Use Study.
This project is the largest case-control study to examine the risk of a young person developing brain cancer in relation to his/her exposure to electromagnetic fields and wireless radiation from mobile phones. This 14-nation case-control study was funded by the European Commission (EC) from March 2009 to February 2016. The EC contributed 58% of the total budget for this €6.1 million ($7.4 million) project. The EC funding for this 7-year project ended five years ago!
Was mobile phone use associated with increased risk of brain tumors or neurological disorders among these youth?
—
Clinical presentation of young people (10-24 years old) with brain tumors: results from the international MOBI-Kids study
Angela Zumel-Marne et al. Clinical presentation of young people (10-24 years old) with brain tumors: results from the international MOBI-Kids study. J Neurooncol. 2020 Apr;147(2):427-440. doi: 10.1007/s11060-020-03437-4. Epub 2020 Mar 3. DOI: 10.1007/s11060-020-03437-4.
Abstract
Introduction: We used data from MOBI-Kids, a 14-country international collaborative case-control study of brain tumors (BTs), to study clinical characteristics of the tumors in older children (10 years or older), adolescents and young adults (up to the age of 24).
Methods: Information from clinical records was obtained for 899 BT cases, including signs and symptoms, symptom onset, diagnosis date, tumor type and location.
Results: Overall, 64% of all tumors were low-grade, 76% were neuroepithelial tumors and 62% gliomas. There were more males than females among neuroepithelial and embryonal tumor cases, but more females with meningeal tumors. The most frequent locations were cerebellum (22%) and frontal (16%) lobe. The most frequent symptom was headaches (60%), overall, as well as for gliomas, embryonal and ‘non-neuroepithelial’ tumors; it was convulsions/seizures for neuroepithelial tumors other than glioma, and visual signs and symptoms for meningiomas. A cluster analysis showed that headaches and nausea/vomiting was the only combination of symptoms that exceeded a cutoff of 50%, with a joint occurrence of 67%. Overall, the median time from first symptom to diagnosis was 1.42 months (IQR 0.53-4.80); it exceeded 1 year in 12% of cases, though no particular symptom was associated with exceptionally long or short delays.
Conclusions: This is the largest clinical epidemiology study of BT in young people conducted so far. Many signs and symptoms were identified, dominated by headaches and nausea/vomiting. Diagnosis was generally rapid but in 12% diagnostic delay exceeded 1 year with none of the symptoms been associated with a distinctly long time until diagnosis.
Open access paper: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7136306/
—
January 26, 2019
The MOBI-Kids project is the largest case-control study to examine the risk of a young person developing brain cancer in relation to his/her exposure to electromagnetic fields and wireless radiation from mobile phones.
The study was funded by the European Commission from March, 2009 to February, 2016. The EU contributed 58% of the total budget for this €6.1 million project.
Although the EU project ended three years ago, the authors have not yet published the most important outcomes from this study.
Following is the executive summary from the authors’ final report to the European Commission:
Final Report Summary: MOBI-KIDS (Risk of brain cancer from exposure
to radiofrequency fields in childhood & adolescence)
Executive Summary
“The overall objective of the current project was to assess the potential carcinogenic effects of childhood and adolescent exposure to radio frequency (RF) and extremely low frequency (ELF) from mobile telephones on tumours of the central nervous system.
In order to achieve this, the operational objectives were:
– To conduct a multinational epidemiological case-control study of brain tumours diagnosed in young people in relation to electro-magnetic fields (EMF) exposure from mobile telephones and other sources of RF in eight countries under the current grant, and, subject to funds being secured separately, in a number of non-European countries;
– To develop and validate improved indices of RF and extremely low frequency (ELF) exposure, and assess related uncertainties, for all subjects in the study;
– To analyse the relation between risk of brain tumours and exposures to RF and ELF from mobile phones and other relevant and important sources of exposure in young people’s general environment.
The MOBI-KIDS project was conducted in 14 countries (Australia, Austria, Canada, France, Germany, Greece, India, Israel, Italy, Japan, Korea, New Zealand, Spain, The Netherlands) between 2010 and 2015. It used a case-control study design, recruiting 898 eligible cases aged 10 to 24 years old and 1 912 controls matched to the cases on reference date, study region and age.
Each participant completed a face-to-face interview that included information on socio-demographic factors; complete residential history; exposure to farm and domestic animals; mobile phone use; use of other wireless communication devices including cordless phones and Wi-Fi; exposure to other environmental and occupational sources of EMF; occupational history of the subject and his/her parents during the peri-conception, pregnancy and peri-natal period; occupational exposures to ionising radiation and chemicals; medical radiation exposure; medical history of the subject and mother and water and disinfection by-products exposure (the later only in 6 countries). Interviewers completed a questionnaire regarding responsiveness of the interviewee and quality of recall.
Validation studies were conducted, as well as various sub studies, to assess the validity and accuracy of the information collected and identify and characterise possible recall and selection biases which may affect the interpretation of study results. Extensive work went into characterising, modelling and validating ELF and RF exposure from different types of mobile and cordless phones, different communication systems and other environmental sources of EMF. The mobile and cordless phones ELF and RF algorithms, to estimate amount of exposure at the location of the tumour, have been completed and validated. Estimation of occupational and environmental exposures to EMF and other factors is underway.
Most brain tumours were of the neuroepithelial type mainly gliomas. Mean age of cases and controls at the reference date is 16.53 and 16.67 respectively with 56% of male participants. There were similar proportions of childhood (10-14) adolescent and young adult cases and controls. Tumour localisation was made by neuro radiologists in each country using standardised age-specific 3D grids for over 90% of cases. Validation of tumour localisation and of diagnosis is underway.
Among regular users of mobile phones, the mean time since start of mobile phone use was 6.2 years for controls, with high differences by age group: 3.2 years for the younger age group (10-14) and 9.2 years for the older age group (20-24), respectively; in the latter group, 37% of controls reported using a phone for 10 years or more. Average number of calls per month was 43 for cases and 49 for controls – with 5% of cases and 4% of controls making more than 10 calls per day on average –, and average hours per month talking on the mobile phone were 2.1 and 2.6 respectively – 4% of case and 3% of controls used the phone for calling more than 1 hour per month on average. In both indicators of mobile phone use, we observed an increasing trend in number of calls and average call time with age.
Analyses of the association between mobile phone use and brain tumour risk, as well as between estimated RF and ELF exposure at the location of the tumour and risk of brain tumour have been conducted and a publication is in preparation. Results however cannot be made public until publication in a peer-reviewed scientific journal.
This is by far the largest epidemiological study on the effects of EMF on brain tumour risk in young people.”
Funded by European Commission FP-7/Environment grant agreement: 226873
Project start date: March 1, 2009
Project end date: February 29, 2016 (closed project)
Overall budget: € 6 078 765,80
EU contribution: € 3 499 748
More information: https://cordis.europa.eu/project/rcn/89894/reporting/en
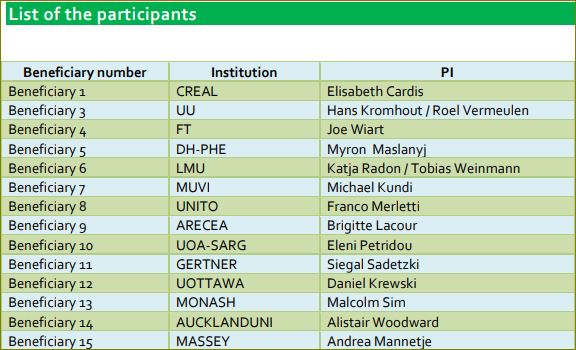
Grant Recipients
Feb 1, 2017
Research on the adverse effects of mobile phone radiation has focused on the radiofrequency (RF) emissions from cell phones and cordless phones and has ignored the effects of the extremely low frequency fields (ELF) produced by the phones. Yet ELF was labelled “possibly carcinogenic to humans” by the WHO International Agency for Research on Cancer a decade earlier than RF.
The paper below indicates that the MOBI-Kids research team is studying the effects of exposure to ELF as well as RF on children’s cancer risk from mobile and cordless phone use.
ELF exposure from mobile and cordless phones
for the epidemiological MOBI-Kids study
Calderón C, Ichikawa H, Taki M, Wake K, Addison D, Mee T, Maslanyj M, Kromhout H, Lee AK, Sim MR, Wiart J, Cardis E. ELF exposure from mobile and cordless phones for the epidemiological MOBI-Kids study. Environ Int. 2017 Jan 23. pii: S0160-4120(17)30047-8. doi: 10.1016/j.envint.2017.01.005. [Epub ahead of print]
Abstract
This paper describes measurements and computational modelling carried out in the MOBI-Kids case-control study to assess the extremely low frequency (ELF) exposure of the brain from use of mobile and cordless phones. Four different communication systems were investigated: Global System for Mobile (GSM), Universal Mobile Telecommunications System (UMTS), Digital Enhanced Cordless Telecommunications (DECT) and Wi-Fi Voice over Internet Protocol (VoIP). The magnetic fields produced by the phones during transmission were measured under controlled laboratory conditions, and an equivalent loop was fitted to the data to produce three-dimensional extrapolations of the field. Computational modelling was then used to calculate the induced current density and electric field strength in the brain resulting from exposure to these magnetic fields. Human voxel phantoms of four different ages were used: 8, 11, 14 and adult. The results indicate that the current densities induced in the brain during DECT calls are likely to be an order of magnitude lower than those generated during GSM calls but over twice that during UMTS calls. The average current density during Wi-Fi VoIP calls was found to be lower than for UMTS by 30%, but the variability across the samples investigated was high. Spectral contributions were important to consider in relation to current density, particularly for DECT phones. This study suggests that the spatial distribution of the ELF induced current densities in brain tissues is determined by the physical characteristics of the phone (in particular battery position) while the amplitude is mainly dependent on communication system, thus providing a feasible basis for assessing ELF exposure in the epidemiological study. The number of phantoms was not large enough to provide definitive evidence of an increase of induced current density with age, but the data that are available suggest that, if present, the effect is likely to be very small.
https://www.ncbi.nlm.nih.gov/pubmed/28126406
May, 2016
According to the European Commission, the EU-funded project “Risk of brain cancer from exposure to radiofrequency fields in childhood and adolescence” (MOBI-Kids) was “closed” on Feb 29, 2016. The study will make an important contribution to assessing the association, if any, between electromagnetic field exposure due to use of mobile communication devices and the development of brain cancer in youth.
The last Mobi-Kids Consortium meeting was held February 16-17, 2016. The meeting was attended by investigators from 15 countries. Preliminary results from the study were discussed.
From December, 2010 through February, 2015, about 800 cases and 1,600 controls were interviewed for this study.
The project cost 6 million Euros with 3.5 million Euros from the European Commission.
June, 2014
My comments:
This is a difficult case-control study to undertake as it involves 14 nations and about 60 senior investigators. The original goal was to recruit 2,000 cases. The authors revised the original goal to 1,000 cases because recruitment of cases has been much more difficult than anticipated. As of June, 2014, only 686 cases were recruited, and 566 were interviewed. Only six more months remain for participant recruitment. Thus, even the reduced recruitment goal may be difficult to achieve.
I am concerned that the MOBI-Kids study will fail to have adequate statistical power to detect the association between EMF exposure and brain tumor risk. The CEFALO study of brain tumor risk in children was seriously under-powered with 352 cases (Aydin et al., 2011; http://bit.ly/1pW4ulA). The four nation CEFALO study found a 36% increased relative risk of brain tumors with any mobile phone use, but this was not statistically significant due to the small sample size (OR = 1.36; 95% CI = 0.92 to 2.02) so the authors dismissed this overall finding. (See my supplementary comments below because CEFALO found some statistically significant evidence for increased brain tumor risk which the study authors also dismissed.)
Only four of the 58 authors of the MOBI-Kids study declared conflicts of interest (see below). The funding sources for this study are listed below. I will leave it to others to determine how much of the funding originated from industry and whether funneling the funds through intermediary organizations or agencies eliminated potential conflicts of interest.
Activist Post reports regularly about wireless phones and other unsafe technology. For more information visit our archives and the following websites:
- Electromagnetic Radiation Safety
- Environmental Health Trust
- Physicians for Safe Technology
- Wireless Information Network
Become a Patron!
Or support us at SubscribeStar
Donate cryptocurrency HERE
Subscribe to Activist Post for truth, peace, and freedom news. Follow us on SoMee, Telegram, HIVE, Flote, Minds, MeWe, Twitter, Gab, What Really Happened and GETTR.
Provide, Protect and Profit from what’s coming! Get a free issue of Counter Markets today.
Be the first to comment on "Experts Conclude Results Reported in Study on Kids’ Wireless Phone Use and Brain Tumor Risk “should be dismissed”"