

Sayer Ji, Contributor
Activist Post
The “diseases of affluence,” as they are known, include diabetes, heart disease, arthritis, osteoporosis and cancer, and are sometimes referred to as the “Western disease” paradigm. They emerge largely in response to the type of overnourishment that occurs in relatively wealthy societies, and particularly the excessive consumption of certain evolutionarily incompatible foods that nonetheless have become the nutritional centerpiece of agrarian, grain-based cultures. (Consider that we have only been consuming the seeds of cereal grasses, i.e. grains, en masse for 10-20,000 years, which while ancient in cultural time, is but a nanosecond in biological time!)
While we have already spent considerable time indicting the credibility of wheat as a so-called health food, whose secular and religious glorification are unparalleled within the cereal grains, we have not delved deeply enough into the link between grain consumption, particularly wheat, and cardiovascular disease, the #1 cause of death in the Western world.
This link, of course, strikes literally to the heart of the seemingly indestructible myth that eating wheat, and more exactly whole wheat (which has more lectin than white, processed wheat flour), is a good thing for human health. Beyond the well over 200 adverse health effects linked to wheat consumption that now exist in the peer-reviewed biomedical literature, we hope to point out in the following article how cardiovascular health is better served by eliminating this uniquely problematic grain from the diet.
It was actually Loren Cordain, Ph.D., author of the Paleo Diet, who (to our knowledge) first pointed out the inherent cardiotoxicity of wheat. In the March 2008 edition of The Paleo Diet Newsletter, Cordain explains in an article titled, “Whole Wheat Heart Attack Part 2: The Role of Dietary Lectins,” how dietary lectins, as found in wheat, promote the formation of fatty streaks and mature atherosclerotic plaque in the arteries.
First, he explains how dietary lectins, which we like to call “invisible thorns” within many commonly ingested plant foods, and which are designed to fend off microbial and animal predators (among other functions), are capable of gaining entry into the circulatory system:
In order for dietary lectins to be promoters of atherosclerosis, the following physical and physiological processes must occur: 1) must survive cooking and processing; 2) they must survive dig enzymatic degradation; 3) they must bind gut tissue; 4) they must cross gut tissue barrier; 5) they must resist immunological and hepatic (liver) disposal; 6) they must arrive in peripheral circulation intact in physiological concentrations; 7) they must interact with one or more mechanisms known to influence atherosclerosis. The six of these seven steps are known to transpire, as ingested lectins rapidly appear intact in the bloodstream of humans and animals and cross the intestinal barrier in human cultured tissue.
Second, he asks the question:
So, we know that dietary lectins can get into the bloodstream of humans and animals, and we know that chronic, low-level inflammation is essential for all facets of atherosclerosis. Is there any evidence that lectins are involved in the progression or acceleration of atherosclerosis? Further, is there any evidence that dietary lectins may promote chronic, low level inflammation in humans?
In answer, he first discusses the well-known atherosclerosis-promoting effects of peanut lectin, as well as the intriguing fact that atherosclerosis almost always occurs, not just anywhere, but in a specific location of the arteries. Basically, at sites where arteries branch a protective glycocalyx (a wispy, hairy structure whose “slipperiness” reduces turbulent flow) prevents damage that might otherwise be caused by white blood cells attaching to adhesion molecules on the surface of the cells lining the arteries. The attachment of white blood cells and subsequent infiltration of the middle section of the artery — namely, the intima media — by them, is what leads to the formation of fatty streaks within the arteries, eventually leading to plaque formation which may obstruct the flow of blood within the narrowing lumen of the artery. Therefore, when the glycocalyx is disturbed, and/or excessive glycocalyx shedding there is induced — presumably by dietary lectins like wheat lectin — the resulting increased arterial wall shear stress and inflammation contributes to atherosclerosis.
For a more elaborate and technical explanation of the process, Cordain explains the process below:
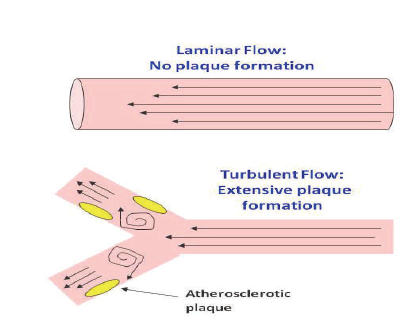
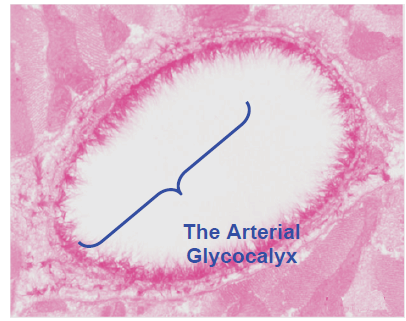
Plaques only form in turbulent flow areas along the artery, such as sites where arteries branch (Figure 1, below), but not where blood flow is smooth (laminar flow), such as in small arteries and at non-branching or non-curving sites. Until recently, the mechanisms underlying this phenomenon was poorly understood. Let’s again examine the artery cross-section shown in Figure 2 (below) and take a more detailed look at the true structure lining the inside of arteries, the glycocalyx. This wispy, hairy structure is composed of sugars and carbohydrate molecules that form a physical barrier between the red and white blood cells in circulation and the endothelial cell surface, thereby preventing white blood cells from attaching to adhesion molecules. In other words, one of the very first steps in atherosclerosis, the entry of monocytes into the intima, is blocked when the glycocalyx is fully intact17. Only when the glycocalyx mass is reduced can monocytes and T-cells bind adhesion molecules and find their way into the intima. Turbulent flow areas are more susceptible to atherosclerosis because the glycocalyx mass is reduced in these areas18. It is known that high-fat diets (which increase the rate of oxidized LDL formation) cause the glycocalyx size and mass to be reduced 18, as do inflammatory cytokines19. From a physiological perspective, reductions in glycocalyx size and mass in response to injury or inflammation make sense. Shedding of the glycocalyx allows the white blood cells entry to the inflamed tissue from circulation and therefore begins the healing process by first destroying and then taking up the foreign substance.
Common dietary lectins are potent stimulators of inflammatory cytokines in white blood cell cultures20,21. In Figure 3 you can see that lectins from lentils, kidney beans, peas and wheat potently increase the production of inflammatory cytokines (IL-12, IL-2, and INFγ). Wheat lectin (WGA) also stimulates production of two other inflammatory cytokines (TNFα and IL-1β)21 that promote the atherosclerotic process. Consequently, if dietary lectins reach circulation intact, which previous human and animal studies demonstrate1-5, they have a high probability of causing glycocalyx shedding, thereby increasing entry of monocytes into the intima and contributing to the formation of the fatty streak. Because of their potent inflammatory nature, dietary lectins have the potential to promote and accelerate atherosclerosis at all steps of this disease where inflammatory cytokines are operative. You will recall that one of the deadly steps involved in atherosclerosis is the rupturing of the fibrous cap and the formation of a blood clot. Enzymes called matrix metalloproteinases (MMPs), secreted by white blood cells and other cells within the plaque, are known to cause collagen and elastic tissue within the fibrous cap to disintegrate.
Consequently, any dietary or environmental factor which facilitates synthesis of MMPs is not a good thing for cardiovascular disease patients. Well guess what? Lectins from wheat, WGA22, and lectins from kidney beans, PHA23, cause tissue cultures of white blood cells to increase their production of MMP
Wheat lectin, also known as Wheat Germ Agglutinin (WGA), is highly selective in what it binds to (the word select and lectin share the same etymological root), and has such a high affinity with certain biomolecules that make up the glycocalyx – n-acetyl-glucosamine and sialic acid – that the problem with lectin-arterial glyocalyx distruption is clear as day. Just as wheat lectins bind to the slippery mucous coat of the glycocalyx in the intestines, contributing to their well-known gastrointestinal toxicity, once they enter into systemic circulation, they may also bind to the slippery glycocalyx lining the arteries, resulting in the damage and subsequent inflammation associated with atherosclerosis.
According to Cordain, another way in which wheat germ agglutinin contributes to the final and fatal step in atherosclerosis, is through its agglutinating effect, i.e. “to cause to adhere, as with glue,” which is to say, forming a clot. According to Cordain:
Integral to the formation of clots are platelet cells, which circulate in the bloodstream.Platelets are normally activated when they contact collagen from a damaged blood vessel. WGA directly causes the activation of platelets and potently increases their aggregation (clumping) 24. Hence, the consumption of whole wheat may be integral in the thinning and destruction of the fibrous cap as well as the formation of the fatal clot.
The ability of lectins to cause the clumping up of cells in the plasma is well known. The Eat Right For Your Blood Type system, for instance, is based upon ascertaining the agglutinizing effects of different foods on different blood types. If wheat lectin can contribute both to inflammation in the lining of the arteries, and cause clumping up and clotting of the blood, there is little doubt that it can also contribute to the #1 cause of death in the Western world. There is also the possibility that the immune system may respond to the presence of wheat proteins by producing antibodies that cross-react with cardiovascular tissue, causing myocardial inflammation, i.e. myocarditis. Myocardititis was in fact identified to be a potential cause of autoimmune myocardititis in a minority of celiac disease patients.1
Resources
1 Andrea Frustaci, Lucio Cuoco, Cristina Chimenti, Maurizio Pieroni, Giuseppina Fioravanti, Nicola Gentiloni, Attilio Maseri, Giovanni Gasbarrini. Celiac disease associated with autoimmune myocarditis.Circulation. 2002 Jun 4;105(22):2611-8. PMID: 12045166
This article first appeared at GreenMedInfo. Please visit to access their vast database of articles and the latest information in natural health.

linkwithin_text=’Related Articles:’
Be the first to comment on "Wheat Toxicity: As Serious As A Heart Attack"